{kind=link}
Connect with us:






Bare minimum spending increases on Australian health infrastructure destroyed by decades of budget slashing, shutdowns and corporatisation is a dangerous charade. The disaster in healthcare has been acute for some time but the addition of a new threat, namely COVID-19, is revealing exactly how dire it is. It is this vulnerability, not only the tenuous state of Australia’s inadequate hotel quarantine system, that has authorities on edge about importing COVID cases among Australians returning from India, leading to drastic actions to shut them out.

The stripping of health infrastructure went into high gear in the 1990s with the onset of a major policy shift to economic rationalism dictated by the Mont Pelerin Society (MPS) network of international think tanks, sponsored by the City of London financial oligarchy. In 1998 the Citizens Party published a pamphlet, Australia’s healthcare ‘reforms’: A Nuremburg crime against humanity, which exposed how economic rationalism, pushed by Liberal Prime Minister John Howard (1996-2007) and exemplified by Victoria under Liberal Premier Jeff Kennett (1992-99), threatened the lives of Australians due to the growing denial of adequate medical care. One of the lead authors of the healthcare reforms, former senior Commonwealth Treasury official Des Moore, a senior fellow at MPS think tank the Institute of Public Affairs, called for a “major downsizing in the Victorian health Department”, paired with “a move to a competitive market situation”.
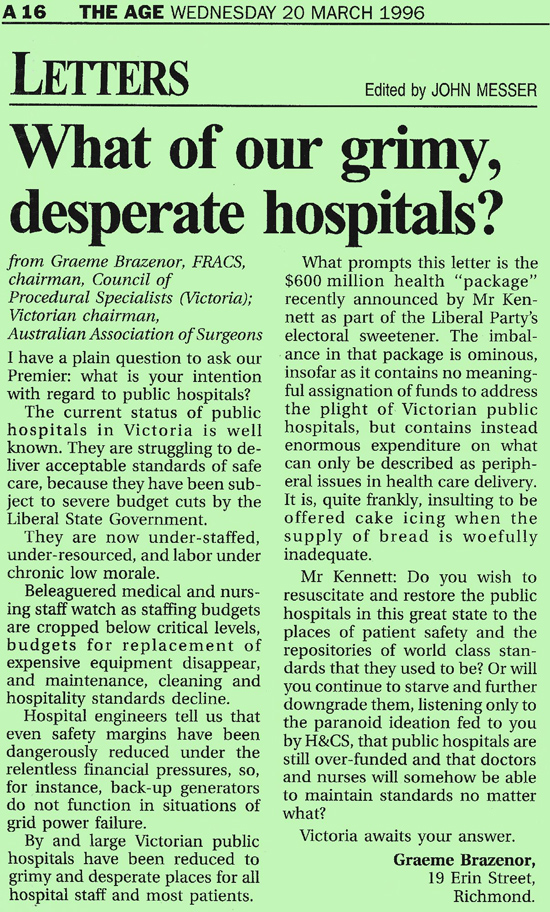
While Federal Health Minister Dr Michael Wooldridge claimed there were too many doctors in Australia and cut the number of new healthcare provider places, the Citizens Party pamphlet called for increased healthcare resources for a period in which “old diseases are resurfacing and becoming ever more virulent, and new, species-jumping forms of deadly viruses are making their appearances”. The pamphlet cited Dr Graeme Brazenor, Senior neurosurgeon at Melbourne’s Austin and Repatriation Hospitals, who denounced Kennett’s budgets as cutting “down to the bone and … starting to demolish the system”. If the state public hospital system “was a dog”, he said, “you’d shoot it”. He resigned in 1997 after six surgery patients were infected with golden staph, saying, “I will not be party to a standard that is as sick as this.”
The Citizens Party followed up in 2002 with a New Citizen feature, “Rebuild the Health System!” The hospital system was so bad that the 4 November 2001 Western Australian newspaper the Sunday Times reported that “plans have been discussed to erect tents for times when all three major Perth hospitals are forced to turn ambulances away”. A senior medical official at Sir Charles Gairdner Hospital, after apologising for the death of an elderly woman in a hospital corridor, was quoted: “We struggle to deal with an extra five patients, let alone another 150 from a train crash. … [I]f there was a major disaster in Perth we would melt down.”
Nationwide, from 1980 to 2016-17 acute care hospital beds nearly halved, from 6.4 to 3.8 per thousand population. Ambulance officials in both Melbourne and Sydney recently revealed the dangerous situation at hospital emergency departments. Ambulance Victoria chief operating officer Mark Rogers, according to the 21 April Age, reported that as ambulance response times worsened in 2021 emergency protocols have been adopted at triple the rate compared with the previous two years combined. Victorian emergency medicine specialist Sarah Whitelaw told the paper there was “an acute public health disaster”, with the system at its worst in three decades: “We haven’t understood how close we were to a crisis before COVID with normal demand outweighing health system capacity”, she said, adding, “We are incredibly nervous going into winter. Even with no COVID, no flu … we are tipping over the edge.”
This is due not only to overcrowded emergency rooms (due to a variety of factors, but nonetheless occurring in the absence of any extraordinary public health crisis), but also to shortages of staff and beds. And with ambulances “ramped” at hospital concourses for hours, there is a shortage of vehicles for new callouts, with patients often advised to take a taxi. “I think we’ve actually passed the tipping point”, said Victorian Ambulance Union secretary Danny Hill.
A NSW Ambulance inspector told the 30 April Sydney Morning Herald that the Sydney ambulance network went to the highest level emergency-response mode in late April, requiring educators, managers and new graduates to join response teams. Response times blew out, from a target of ten minutes for cardiac arrest to 45, for instance. The ambo said he had not seen the system under such strain in his 20 years on the job, warning winter is looking “very ugly”. Staff are so exhausted they can’t be convinced to take an extra shift for double the money, Kogarah intensive care paramedic Brett Simpson told the paper.
Queensland Health Minister Yvette D’Ath pointed to a similar crisis in her state, news.com.au reported, with hundreds of aged and disabled patients who should be in dedicated care facilities taking up hospital bed capacity. Australian College for Emergency Medicine spokesperson Kim Hansen described it as the worst situation emergency doctors had ever experienced, their efforts akin to “putting a Band-Aid on a stab wound”.
The NSW and Victorian governments cited increased funding for ambulance services; but after decades of stripping public health facilities, money alone will not work. In a March 1996 letter published by The Age, Dr Brazenor had denounced a Kennett election “sweetener” in the form of a $600 million health package as directed into “peripheral” health expenditure with no meaningful impact on public hospitals. He mentioned beleaguered staff, reduced safety margins and failing equipment. Today, an ongoing inquiry by the NSW parliament into health services in remote and regional areas is turning up damning consequences of lack of staff and basic supplies, including unnecessary deaths. Only nine of 38 hospitals in the western part of the state, for instance, carry blood supplies.
Health funding has increased modestly in recent years, but is nowhere near sufficient to overcome the combination of a growing and aging population, inflation, and the accumulated deficit of basic services, trained staff and infrastructure. Furthermore, an increasing proportion of revenue is spent on external consultants. In the 22 years from 1997-98 to 2019-20, the amount of money spent on consultancies—outsourcing various health roles and decision-making to private executives on fat pay packets—nearly tripled. It nearly doubled in the six-year subset from 2013-14 to 2019-20.
The 1997-98 Commonwealth Health Department Annual Report referenced its adherence to the agenda of “major structural reforms … aimed at reducing the rate of growth of spending across the portfolio to more sustainable levels”. This included a pathway “to establish a successful framework for outsourcing” and guidelines for outsourcing in order to concentrate on “core functions”, completed that year under National Competition Principles.
The covert privatisation and outsourcing of vital public health services must be immediately reversed and proper care standards restored.
By Elisa Barwick, Australian Alert Service, 12 May 2021